
Peptides are having a moment. About 10 million searches a month in the US now. This spring I stopped searching and ran one on myself: retatrutide, the strongest one in the trial data so far.
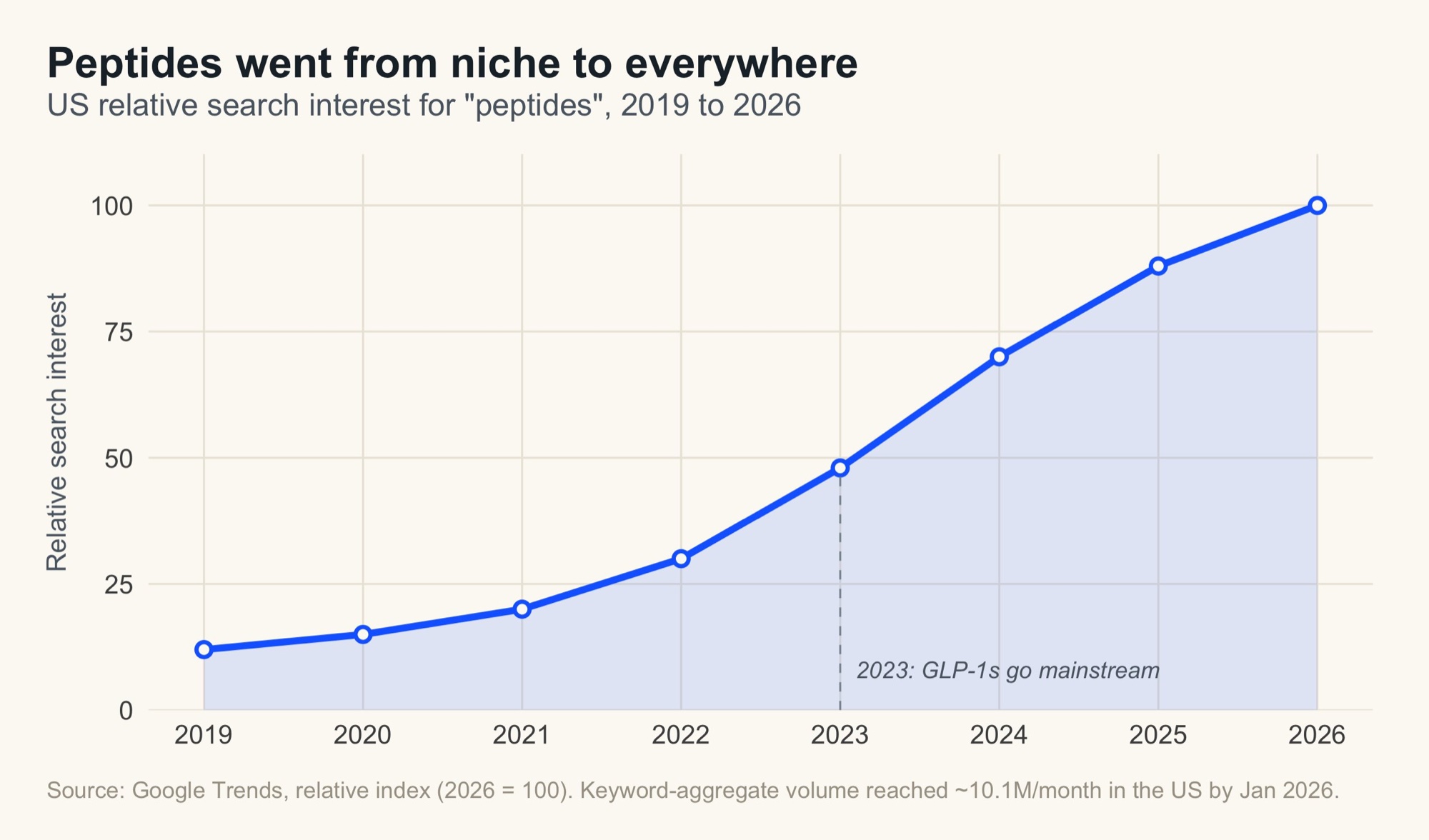
They're not new, though. Insulin, the first peptide we ever turned into medicine, has kept people alive since 1922[1]. Ozempic, the one that made the whole class a household name, only landed in 2017[2]. Reta is the newest of the line, and the most powerful yet.
Mine was two shots over two weeks, then I stopped. It worked, that was never the problem. The problem was that the most obsessive health setup I could build still couldn't answer the one question that mattered. Here's what actually happened.
What it is, fast
Quick bit of science, and I'll keep it painless.
Your body already runs on peptides. Insulin is one. Ozempic is one too. They're short chains of amino acids your body uses as signals.
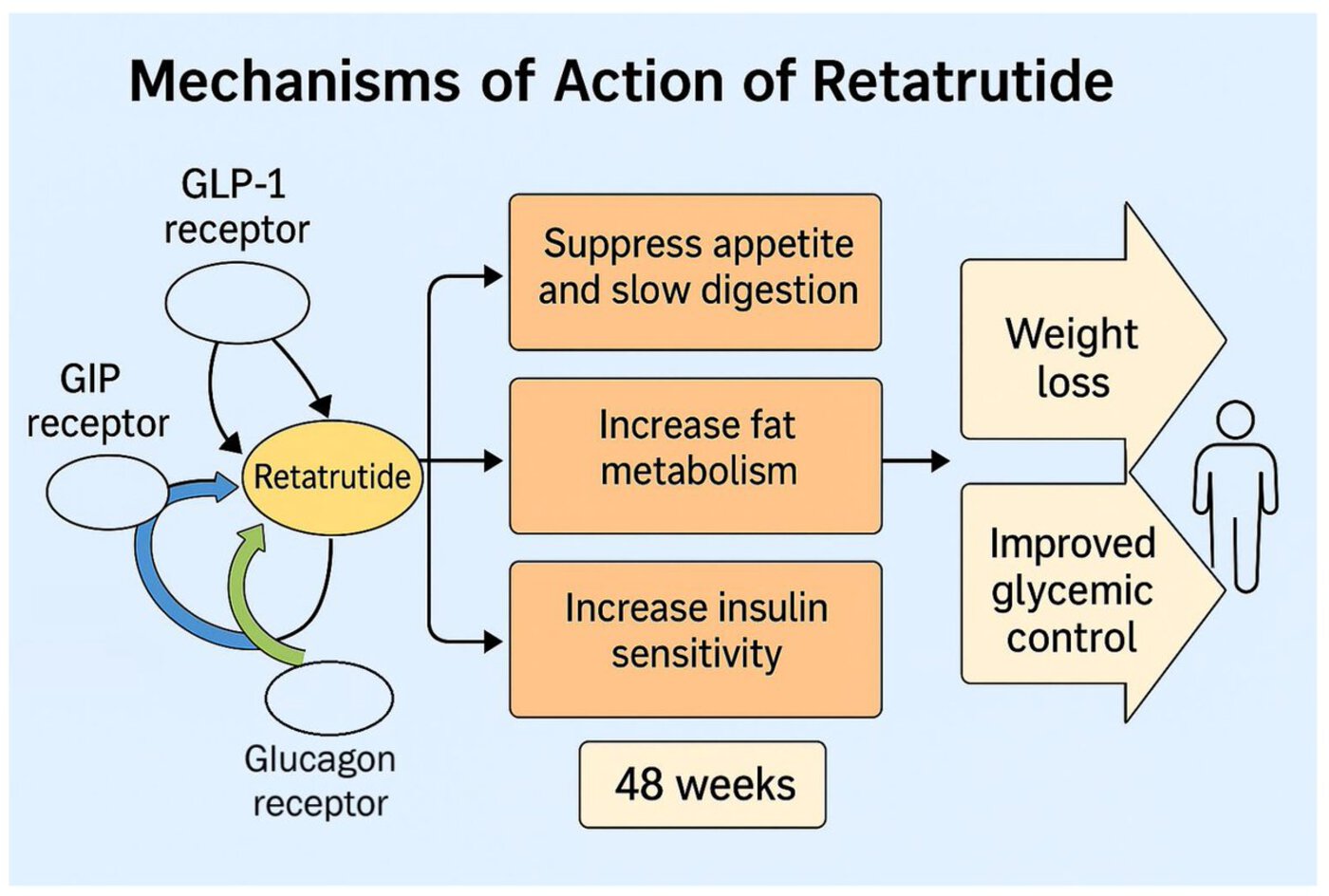
Ozempic mimics GLP-1, a gut hormone that tells your brain you're full. Natural GLP-1 burns off in minutes; the drug makes it last a week. Mounjaro added a second signal. Reta adds a third, glucagon[3]. That one is the leading explanation for why it out-loses the others: it seems to push your liver to burn more at rest, so it touches what you burn, not just what you eat.
The trial numbers, because they matter: in the phase 2 obesity trial reta dropped about 24% of body weight at 48 weeks[4], and the curve still hadn't flattened when the trial ended. In diabetics it's lower, around 15%[3]. Population and duration move the number a lot, anyone quoting one figure hasn't read past the headline.
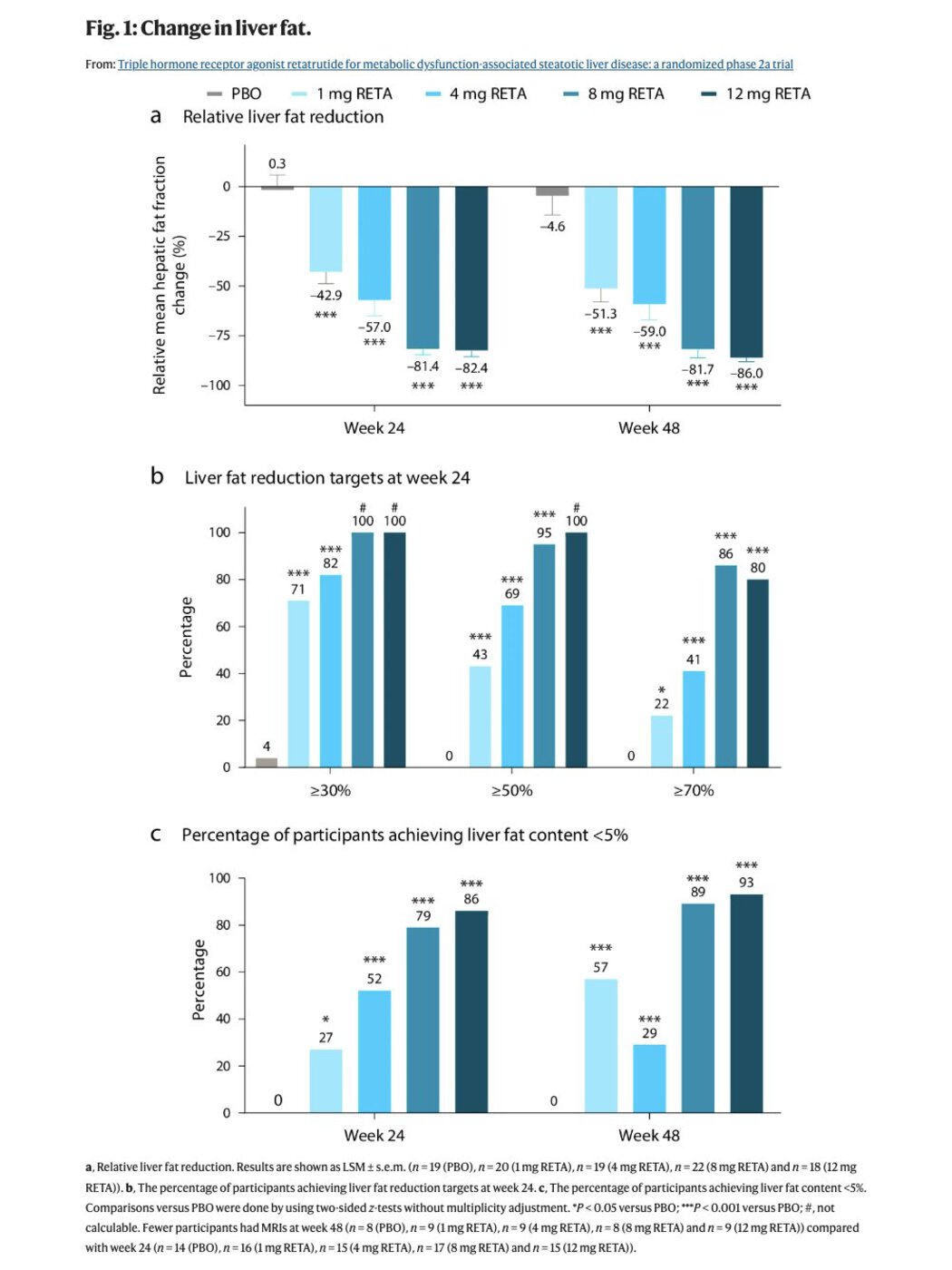
What pulled me in wasn't just the weight, it was both. In those same trials it also cut liver fat by around 86%[5] and pulled most prediabetics back to normal blood sugar. Fatty liver hits 40% of the world.
And that's just what's proven. It's being studied for heart and kidney disease, and, stranger, for dialing down compulsion, more on that below.
This is a metabolic drug that happens to also make you lean. The weight might end up the least interesting thing it does.
Why I did it
Three reasons, honestly.
One, curiosity. Reta is a metabolic drug, and my metabolism already runs in the top 10 to 20%:
- Blood sugar low and steady (HbA1c under 5%)
- Fasting insulin low (around 2 to 5)
- Triglycerides in the 30s and 40s
So this was never about rescue. The question was simpler: what does the strongest metabolic drug in the world do to a baseline that's already dialed in? Full panel here.
Two, and this is the real one: the reason I can't put a number on. I don't want to think about food all day, and on reta I barely did. The willpower food takes is a tax on everything else, and for me that tax went quiet. You don't notice how much of your head it eats until it's gone.
And it reaches past food. The whole class seems to dial down compulsion: less pull to drink, to scroll, to shop, to gamble. Still just anecdote, but the overlap between dopamine and metabolism might be one of the most under-studied corners of medicine. That's the part I'm actually here for.
Three, vanity. A DEXA the week before put me at 11.2% body fat. I wanted the last stubborn bit, closer to 9%.
It all started with my Health OS
Last month I showed you my Health OS: all my data in one folder an AI reads across. My Whoop, my labs, my DEXA, my genome. I built it to run experiments on myself the way Bryan Johnson does, without his medical team or his millions.
Here's how I actually used it for reta. Three steps.
One, everything in one place: my genome, my blood panels, my body composition, my family history, the daily wearable data. The whole picture in one folder.
Two, a documented safety pass with Claude. Not a vibe check: I hand it all of that and ask, in writing, is there anything in here that says don't touch this? It came back clean, with the reasons logged so I could keep them.
Three, daily logging once I started. Every shot, how I felt, plus the Whoop and weight numbers, flowing back into the same folder each morning. The AI checked each one against my baselines and flagged anything drifting. I didn't have to remember to watch. It watched.
What I knew going in
Two things, and they pulled in opposite directions.
The upside. Everything above. The fat loss, the metabolic wins, the food noise gone.
The catch. Reta seems to cost more muscle than the others. In the data, 37 to 40% of the weight lost was lean mass, versus about 25% on Mounjaro. It's unclear how much is the drug and how much is low-protein, sedentary trial populations. But I was already lean and holding muscle the natural way, daily training and enough protein. So that risk was the whole game for me.
It's the reason people rarely run reta alone. They pair it with something that does the opposite. Usually tesamorelin, a peptide that nudges your body into making more of its own growth hormone. More growth hormone means you hold onto muscle while the fat comes off. Reta burns, tesamorelin protects.
I didn't stack anything. I wanted to see what reta does on its own first.
Getting it is the easy part
This is the question I get more than any other. And it's the scariest part of the whole thing.
Reta isn't approved. You can't walk into a pharmacy and ask for it. So most people buy "research-grade" peptides online, and almost all of it traces back to one place: the Chinese grey market. Unregulated labs, a vial, a label, and not much else.

I wasn't willing to run an unapproved drug blind. So I did it under a doctor I actually know and trust, Dr. Jonathann Kuo at Extension Health, with real medical oversight the whole way, someone I could message the second something felt off.
That's the real gap: not getting the stuff, but knowing it's real, clean, and safe to keep taking. For most people, there's still no good answer.
How I microdosed it
In the trials people work up to 12mg. I started at 1mg a week, a fraction of that. The number wasn't mine to pick, it was Dr. Kuo's call: he'd run reta with his own patients, he had my baseline markers, and he knew what I was after, the metabolic edge, not 50 pounds (23kg) to lose.

I took it in the evening, once a week, so it ramped up overnight and was working by the next day.
And before either shot, I wrote my stop-lines off my own baselines. Not a protocol, mine:
- Resting HR up 8 from my ~44, stop.
- HRV down 25%, stop.
- More than 2kg lost in two weeks, stop.
- Strength down two sessions, stop.
What happened
The food noise went silent. And I mean silent. You just forget to be hungry, which is a strange thing to feel if you've spent your whole life thinking about the next meal. Energy stayed level too, no crash, sharp all day.
On the scale, it came off fast: around 74 down to 71 in the two weeks I was on it, then drifting to 69.7 over the six weeks my scale covers. Almost 4kg in all.
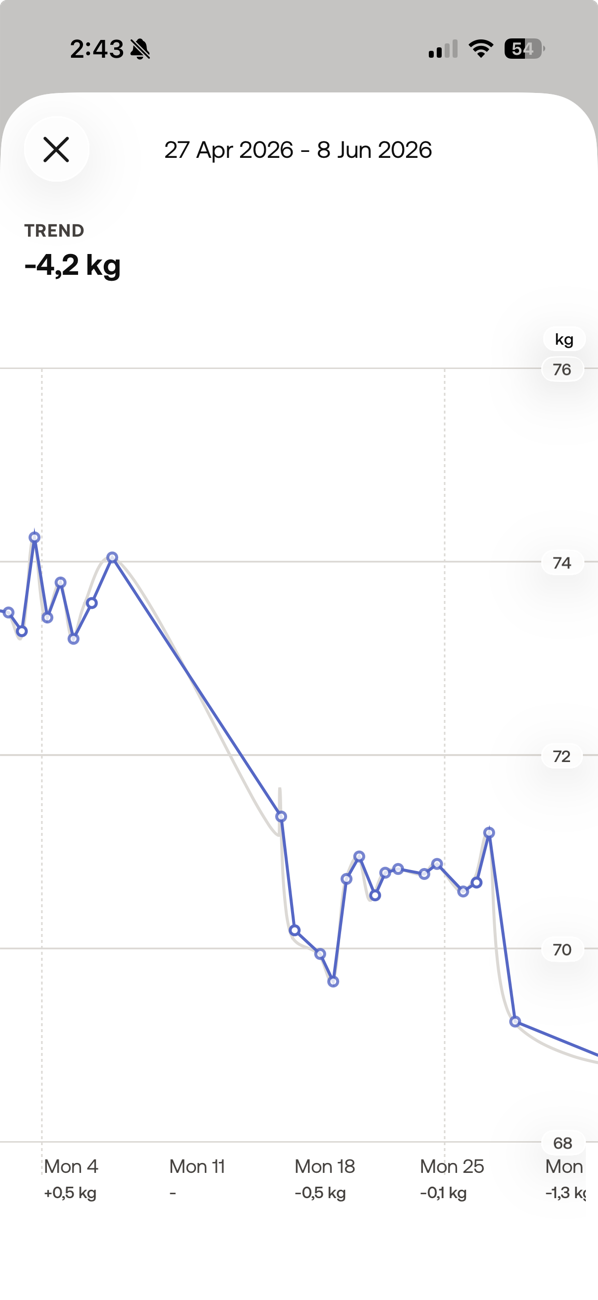
That was the win. It was also the alarm. Three kilos in two weeks blew past my "more than 2kg and I stop" line. Even microdosed, 1mg was too much for my frame. For what I was after, half that, 0.5mg, is where I'd start next time. The right dose for a lean guy holding muscle is nothing like the dose for someone with real weight to lose. There is no one protocol.
Then my Whoop told the fuller story.
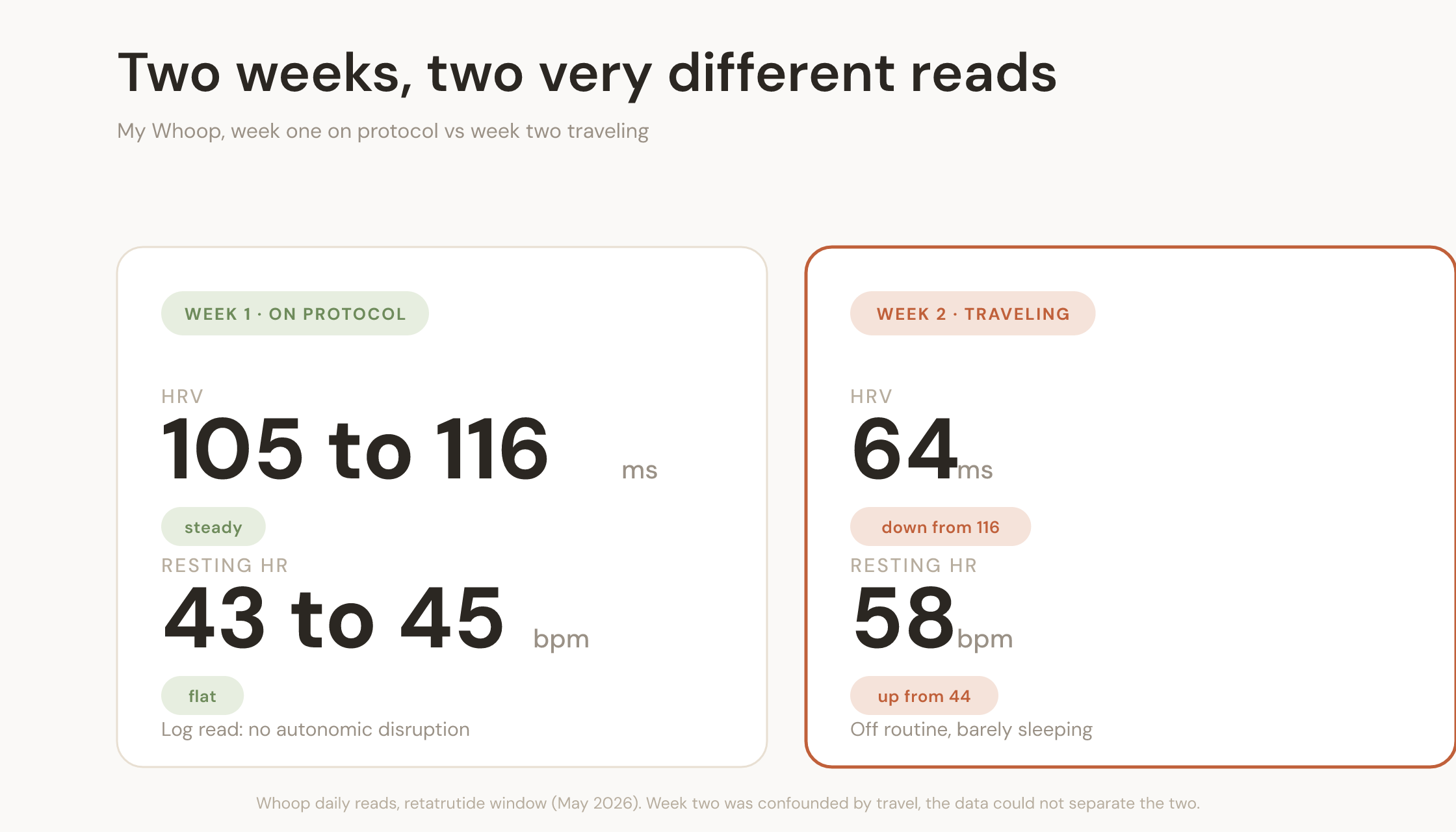
Week one on reta, the clean read: HRV held between 105 and 116ms, resting heart rate flat at 43 to 45. My log literally said "no autonomic disruption." Nothing flagged. It looked calm.
Week two, everything cratered. HRV fell from 116 to 64. Resting heart rate jumped from 44 to 58. That got my attention fast.
Why I stopped
I stopped after two shots. My own stop-lines made the call.
Two of them tripped at once. HRV crashed from 116 to 64, way past my 25% line. And I'd lost almost 4kg, past my 2kg line.
And I couldn't even tell what caused it. That same week I was traveling and barely sleeping, so was the crash the reta or the trip? My data couldn't separate them. That's the wall: it caught the problem, it just couldn't explain it.
I ran it past Dr. Kuo, and we agreed. Two shots, then stop.
What's next
Next I'm testing the ones I'm honestly more curious about than weight loss. Semax and Selank, the focus peptides, to see if I can get a sharp, calm head without the crash you get off stimulants. And CJC, for recovery and holding muscle, the exact thing reta put at risk.
Same method every time. Genetics first. Guardrails off my own baselines. A doctor in the loop. And I'll show you all of it here, the numbers that worked and the ones that didn't, same as I just did with reta.
That's the point of doing this in the open. Not to hand you a protocol, there isn't one. Just to show what it actually looks like to treat your own body like an experiment worth running right.
More soon,
Max
Personal experimentation, not medical advice. Retatrutide is not FDA-approved. This was my baseline and my clinician, not a template. Talk to a doctor before touching any of this.
References
- Leonard Thompson receives the first insulin injection. Toronto, January 1922.
- Ozempic (semaglutide) FDA approval history. First approved December 2017.
- Bajaj HS, et al. Efficacy and safety of retatrutide, a GIP, GLP-1, and glucagon receptor agonist, in people with type 2 diabetes and inadequate glycaemic control with diet and exercise (TRANSCEND-T2D-1), a phase 3 trial. The Lancet, 2026.
- Jastreboff AM, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity, a Phase 2 Trial. New England Journal of Medicine, 2023.
- Sanyal AJ, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease, a randomized phase 2a trial. Nature Medicine, 2024.